Obamacare: Slowly but surely making American citizens, God and George Washington’s special sovereign two-legged creatures, into disposable chunks of meat.
Reporting from Washington — President Obama suggested at a town hall event Wednesday night that one way to shave medical costs is to stop expensive and ultimately futile procedures performed on people who are about to die and don’t stand to gain from the extra care.
In a nationally televised event at the White House, Obama said families need better information so they don’t unthinkingly approve “additional tests or additional drugs that the evidence shows is not necessarily going to improve care.”
He added: “Maybe you’re better off not having the surgery, but taking the painkiller.”
Not quite your “Soylent Green is People!” society…but it’s a big step in that direction.
Obama said he has personal familiarity with such a dilemma. His grandmother, Madelyn Dunham, was diagnosed with terminal cancer and given less than nine months to live, he said.
She fell and broke her hip, “and the question was, does she get hip replacement surgery, even though she was fragile enough they were not sure how long she would last?”
Obama’s grandmother died two days before he was elected president in November. It was unclear whether she underwent the hip-replacement surgery.
The event, hosted by ABC News’ Charles Gibson and Diane Sawyer, gave Obama a prime-time forum to promote his healthcare overhaul. A total of 164 guests were invited. ABC pre-screened questions, though the White House was not made aware of what they would be.
Republicans described the event as an “infomercial,” faulting ABC for giving the president such valuable TV time in the midst of a high-stakes partisan policy discussion.
The audience — which included doctors, patients, health insurers, students and people with ailing relatives — clearly was unhappy with the current healthcare system. Gibson asked for a show of hands to see how many wanted to leave the system unchanged. No one raised a hand.
Ah, the “status quo is unacceptable” argument. Best way to garnish up a bad idea!
I didn’t always think so. Just last winter we were starting to argue hot and heavy about the savings and loan bailout and I wrote to my aging-liberal-hippy-female-ditz senators to tell them how I wanted them to vote, just like I’m supposed to. They wrote back and told me how the vote should go. I think it was Boxer; not entirely sure, it gets hard to tell them apart. Anyway, I was just impressed with how the letter was covered top to bottom, repeating over and over again that the status quo was unworkable and something had to be done.
That worked out just swell, didn’t it?
Maybe…just maybe…that is not exactly the cream-of-the-crop of decision-making methods. “Status quo is unacceptable! I’m going to put sugar in my gas tank!”
In fact — maybe this line of thinking is so conducive to bad decision making, that it’s about to saddle us with a universal healthcare system that our Replacement Jesus isn’t even going to use.
Without question, the most damaging moment for Obama came when he acknowledged that in spite of the rationing implicit in his public health care plan, he would still pay out-of-pocket to obtain the best health care for his family. As reported by ABC’s Jake Tapper, “President Obama struggled to explain today whether his health care reform proposals would force normal Americans to make sacrifices that wealthier, more powerful people – like the president himself – wouldn’t face.”
Though it is not in the standard Republican playbook, the opponents of Obamacare should argue that his program is fundamentally unfair and at odds with America’s egalitarian commitments. Assuming that Republicans are correct, and the creation of a public-plan will lead to the collapse, rather than invigoration, of private health insurance, the end result of Obamacare will be a massive shift from an employer-based system of private health insurance toward government-provided care.
Whether you’re pro-single-payer-healthcare, or anti-, or sitting on the fence wondering what to do…which I suspect most folks are…this is an important point to be pondered. Government health plans always, always, always ration care. Always.
Only by expanding government control of health care can we bring down its cost. That’s the faulty premise of the various proposals for health reform now being batted around Washington. The claimed cost control depends on politically safe ideas such as preventive care or the adoption of electronic health records. And neither — even according to the Congressional Budget Office — will do much to reduce spending.
:
President Obama objects when people use the word “rationing” in regards to government-run health care. But rationing is inevitable if we simply expand government control without fixing the way health care is reimbursed so that doctors and patients become sensitive to issues of price and quality.
Like Medicare’s recent decisions to curtail the use of virtual colonoscopies, certain wound-healing devices, and even a branded asthma drug, the board’s decisions will be one-size-fits-all restrictions. Such restrictions don’t respect variation in preferences and disease, which make costly products suitable for some even if they are wasteful when prescribed to everyone.
Moreover, these health boards prove that policy makers know they’ll need to ration care but want to absolve themselves of responsibility. Some in Congress and the Obama administration recently tipped their hand on this goal by proposing to make recommendations of the current Medicare Payment Advisory Committee (MedPAC) legally binding rather than mere advice to Congress. Any new health board’s mission will also expand over time, just as MedPAC’s mandate grew to encompass medical practice issues not envisioned when it was created.
The idea of an omnipotent board that makes unpopular decisions on access and price isn’t a new construct. It’s a European import. In countries such as France and Germany, layers of bureaucracy like health boards have been specifically engineered to delay the adoption of new medical products and services, thus lowering spending.
In France, assessment of medical products is done by the Committee for the Evaluation of Medicines. Reimbursement rates are set by the National Union of Sickness Insurance Funds, a group that also negotiates pay to doctors.
In Germany, the Federal Joint Committee regulates reimbursement and restrictions on prescribing, while the Institute for Quality and Efficiency in Healthcare does formal cost-effectiveness analysis. The Social Insurance Organization, technically a part of the Federal Joint Committee, is in charge of setting prices through a defined formula that monitors doctors’ prescribing behavior and sets their practice budgets. In the past 12 months, the 15 medical products and services that cleared this process spent an average 35 months under review. (The shortest review was 19 months, the longest 51.)
In short, other countries where government plays a large role in health care aren’t shy about rationing. Mr. Obama’s budget director has acknowledged that rationing reduces costs. Peter Orszag told Congress last year when he headed the Congressional Budget Office that spending can be “moderated” if “diffusion of existing costly services were slowed.”
Medicare can already be painstakingly slow. Appealing to it takes patients an average 21 months according to a 2003 Government Accountability Office report (17 months involve administrative processing). Layers of commissions and health boards would delay access still further.
Obama’s doctor doesn’t agree with Obama on Obamacare:
David Scheiner, an internist based in the Chicago neighborhood of Hyde Park, has a diverse practice of lower-income adults from the nearby housing projects mixed with famous patients like U.S. Sen. Carol Mosely Braun, the late writer Studs Terkel and, most notably, President Barack Obama.
Scheiner, 71, was Obama’s doctor from 1987 until he entered the White House; he vouched for the then-candidate’s “excellent health” in a letter last year. He’s still an enthusiastic Obama supporter, but he worries about whether the health care legislation currently making its way through Congress will actually do any good, particularly for doctors like himself who practice general medicine. “I’m not sure he really understands what we face in primary care,” Scheiner says.
Article Controls
Scheiner takes a few other shots too. Looking at Obama’s team of health advisors, Scheiner doesn’t see anyone who’s actually in the trenches. “I have a suspicion they pick people from the top echelon of medicine, people who write about it but haven’t been struggling in it,” he says.
Scheiner is critical of Obama’s pick for Health and Human Services secretary–Kansas Gov. Kathleen Sebelius, who used to work as the chief lobbyist for her state’s trial lawyers association.
“He doesn’t see all the pain, it’s so tragic out here,” he says. “Obama’s wonderful, but on this one I’m not sure if he’s getting the right input.”
Another recovering Obamabot going through the first stages of remorse.
I had two reactions to the ABC Healthcare Infomercial. First, Gibson’s question about “who likes the status quo” or whatever, was a loaded one, a leading one, and a deceptive one. He could just as well have asked “who has some stories to share about government meddling in things, when it actually worked out well?” With a younger crowd of folks that hadn’t yet put in their decades waiting in line at the DMV, maybe he would’ve gotten some public-school indoctrinated talking points about Franklin Roosevelt ending the Great Depression. But that would be it. Even with a cherry-picked audience full of hardcore liberals, it would be a possibility worth entertaining that all the hands would stay down. How come he asked the question he asked, instead of that one? I’m starting to see Charles Gibson as a walking incarnation of what Thomas Jefferson said about bad information: “The man who reads nothing at all is better educated than the man who reads nothing but newspapers.”
Jefferson knew his subject matter well. I see a talking point has emerged, again, about millions and millions of Americans who lack healthcare [insurance]. Perhaps the time has come to inspect this.
Dr. Eric Novack testified before the House Energy and Commerce’s Subcommittee on Health about the Obama administration’s proposed health care legislation. Afterward, he told CNSNews.com that the Obama administration’s claim that there are 46 million uninsured people in America includes people with different health care scenarios and that combining them togehter in one number is misleading.
“If we start breaking down those numbers a bit–and again these will be round numbers–but about 9 to 10 million of those people are in the country illegally,” Novack said.
Another 15 million are what he called “chronically uninsured,” because of pre-existing health problems or other mitigating factors.
Novack, a self-described “patient advocate” who has written about health reform for the Goldwater Institute and supports legislation in Arizona to protect patients’ right to use and pay for the health care plan of their choice, said another 10 million or so “uninsured” Americans have chosen that status.
“We have young people between 18 and 30, probably about another 10 million or so, they’d rather buy applications for their iPhone than buy health insurance,” Novack said.
He said some of the approximately 46 million Americans referred to by Obama and members of the subcommittee include others who may be eligible for existing government health care programs, such as S-Chip and Medicaid, but don’t sign up.
Hillary and crew were taking the same liberties with the truth fifteen years ago back when the number that was being trotted out was 15 million. They called it “without access to health care,” which could have been called technically correct because if any one of them busted a foot and was hauled into the emergecy room, they’d have to talk to that matronly schoolmarm with the big thick coke-bottle-bottom glasses who would ask to see their health insurance, they’d have none to show, and an awkward situation would develop without this “access to care.” But the foot would have been treated. This, I think, is what Jefferson was talking about.
This is another piece of bad thinking that needs some attention — it’s settled in thick and fast, like fog, since the 1960’s, this notion that if some subclass among us is found to be deprived of something, then on a virtual basis, we all have been so deprived. This is key to Gibson asking who’s happy with the status quo? and seeing not one single hand go up. It is deficient thinking because you could use exactly the performance and exactly the same technique to show the status quo is always unacceptable, with anything. And with the same performance techniques & phony logic, you could then go on to demonstrate that any & all plans carrying that wonderful magic glittering unicorn-phrase of “REFORM,” must be worth trying.
But that isn’t necessarily so.








 So one of the bloggresses we follow, a particularly enchanting and intelligent one, got hold of a phony egghead study that says something completely ridiculous and decided to believe every word in it. Said phony egghead study concerns something men and women are simply not going to see the same way — ever — and it was obviously written up by a chick for other chicks. So don’t be too hard on Dr. Mel, she’s a chick too.
So one of the bloggresses we follow, a particularly enchanting and intelligent one, got hold of a phony egghead study that says something completely ridiculous and decided to believe every word in it. Said phony egghead study concerns something men and women are simply not going to see the same way — ever — and it was obviously written up by a chick for other chicks. So don’t be too hard on Dr. Mel, she’s a chick too. After glasses, there is the height thing. Do you have to stop seeing her if she’s taller? And then the big-nose thing. A lot of guys don’t notice, a lot of other guys can’t stand a big nose on a girl. And then there are the breasts. The arm muscles. Her thighs aren’t curvy enough, or they’re too thin…huge issue for some guys, not worth mentioning to other guys.
After glasses, there is the height thing. Do you have to stop seeing her if she’s taller? And then the big-nose thing. A lot of guys don’t notice, a lot of other guys can’t stand a big nose on a girl. And then there are the breasts. The arm muscles. Her thighs aren’t curvy enough, or they’re too thin…huge issue for some guys, not worth mentioning to other guys.
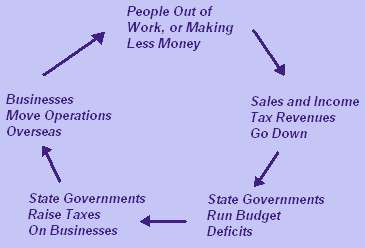 It’s a little irritating if you possess the brainpower to understand the BOHICA Cycle, and can comprehend what’s taking place here. The folks who have a monopoly on power here, are dedicated to making goods and services needlessly expensive for those who depend on themselves to earn the goods and services, and don’t depend on government. They’re using “market forces” to force all commerce to go through the government…and it’s working out just great.
It’s a little irritating if you possess the brainpower to understand the BOHICA Cycle, and can comprehend what’s taking place here. The folks who have a monopoly on power here, are dedicated to making goods and services needlessly expensive for those who depend on themselves to earn the goods and services, and don’t depend on government. They’re using “market forces” to force all commerce to go through the government…and it’s working out just great. Whether we like it or not, it would appear this “skill” is to become the lifeblood of our future generations. I see a tomorrow in which, if you can pull this off, you get to live under a roof, reproduce, and eat; if you can’t then you don’t, don’t and don’t. I see a future in which we systematically ostracize, throughout a process that involves many stages, anyone lacking the ability to do this.
Whether we like it or not, it would appear this “skill” is to become the lifeblood of our future generations. I see a tomorrow in which, if you can pull this off, you get to live under a roof, reproduce, and eat; if you can’t then you don’t, don’t and don’t. I see a future in which we systematically ostracize, throughout a process that involves many stages, anyone lacking the ability to do this. The Federal EPA is about to officially declare carbon dioxide to be a pollutant. That’s not just false and unscientific; it’s not just an excuse for taxing everything in sight, including breathing. It’s not merely wrong. It’s idiotic.
The Federal EPA is about to officially declare carbon dioxide to be a pollutant. That’s not just false and unscientific; it’s not just an excuse for taxing everything in sight, including breathing. It’s not merely wrong. It’s idiotic.
 It’s a pretty tall order. Eco-feminism is inherently incoherent because as a collection of alternative values and scruples, it is designed to oppose something else. And it isn’t willing to admit this. This is why it consists of so many things that are bound together even though they are unrelated. Rather like a homemade kitchen gadget built from oil filters, band-aids, coathangers, silver dollars and cotton swabs. The parts don’t fit together; ecology has very little to do with upholding equal rights and privileges for women.
It’s a pretty tall order. Eco-feminism is inherently incoherent because as a collection of alternative values and scruples, it is designed to oppose something else. And it isn’t willing to admit this. This is why it consists of so many things that are bound together even though they are unrelated. Rather like a homemade kitchen gadget built from oil filters, band-aids, coathangers, silver dollars and cotton swabs. The parts don’t fit together; ecology has very little to do with upholding equal rights and privileges for women.
 You see it in the elections here in the United States. Eight and a half years ago we got a President elected who was viscerally disliked by those who resented manhood — many of whom probably never understood a father’s proper role in the family. They shrieked. Now we’ve got a President who offends the rest of us. We don’t shriek…we groan. Both sides have strong feelings about Presidents disliked, but have dramatically different ways of showing this dislike.
You see it in the elections here in the United States. Eight and a half years ago we got a President elected who was viscerally disliked by those who resented manhood — many of whom probably never understood a father’s proper role in the family. They shrieked. Now we’ve got a President who offends the rest of us. We don’t shriek…we groan. Both sides have strong feelings about Presidents disliked, but have dramatically different ways of showing this dislike.

 In this way, they share a malady with the Obamabots. And they, in turn, with the environmentalists. And all those three, in turn, with all the most powerful progressive-politic types in general. They all have this in common: Meaningless cliches tossed out to suggest something wonderful and grand is being built, but if you watch them across a meaningful length of time you see all they do is destroy things. By now, it’s safe to say that if you don’t have this sickness, you aren’t running anything. Nothing so big that it’s assured to come out on top of things.
In this way, they share a malady with the Obamabots. And they, in turn, with the environmentalists. And all those three, in turn, with all the most powerful progressive-politic types in general. They all have this in common: Meaningless cliches tossed out to suggest something wonderful and grand is being built, but if you watch them across a meaningful length of time you see all they do is destroy things. By now, it’s safe to say that if you don’t have this sickness, you aren’t running anything. Nothing so big that it’s assured to come out on top of things.